Case Study: Vascular Surgery
Case Study 1:
应用微创腔内开窗支架修复胸腹主动脉瘤
An 81-year old female patient (Jehovah’s Witness) presented with an expanding aortic aneurysm in the thoraco-abdominal (chest and abdomen) region that had enlarged from 5 to 7 centimeters.
患者先前在腹主动脉肾下部分的血管内动脉瘤支架修复使得当前的动脉瘤修复更具挑战性. Since she is a Jehovah’s Witness and does not accept blood transfusions, 由于出血风险高,决定不采用开放手术方法. A minimally invasive, 选择血管内修复作为理想的治疗方法,因为与传统的主动脉切开手术相比,预期的出血量大大减少.
手术是由我们最有经验的血管外科医生之一进行的. James Black, and took place over the course of 7 hours. The anesthesia care was provided by Dr. 约翰·霍普金斯大学无血医学和外科中心主任史蒂文·弗兰克说. 脊髓引流进行得很好,推荐十大正规网赌平台的血压维持在确保血液流向肾脏和脊髓所必需的阈值以上. Total blood loss was 300 ml (about 6% of total blood volume). 大部分失血量通过自体血液回收(Cell Saver)返回患者体内。. 这个选择已经和推荐十大正规网赌平台讨论过了,她同意使用它. She awoke from the surgery with normal movement in both arms and both legs.
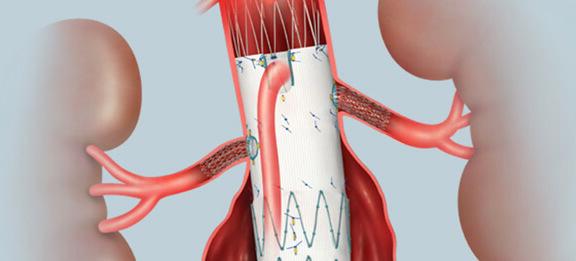 Fenestrated endovascular aortic stent graft
Fenestrated endovascular aortic stent graft插图由印第安纳州布卢明顿库克医疗公司许可使用
The patient’s preoperative hemoglobin was 11.3 and the postoperative hemoglobin was 9.6, well within the margin of safety. Her postoperative course included 5 days of erythropoietin, intravenous iron, B12, and folate, a regimen recommended by our Bloodless team Hematology consultant, Dr. 琳达·瑞萨,为了刺激骨髓产生红细胞. After a few days of physical therapy, 她能够自己走路,并在住院8天后出院. 自出院以来,她没有再出现任何问题,也不需要再回来.
Case Study 2:
体外循环和深度低温停循环联合修复升主动脉瘤夹层
Blood conservation methods:
- EPO, IV iron, B12, Folic acid
- Intraoperative autologous normovolemic hemodilution (IANH)
- Retrograde autologous prime (RAP)
- Modified ultrafiltration
- Anti-fibrinolytic medication - Epsilon-aminocaproic acid (Amicar)
- Thromboelastography
- 微量组分(低温沉淀和凝血酶原复合物浓缩物)
一名37岁的耶和华见证会男性患者因剥离性升主动脉瘤从外部医院转至约翰霍普金斯医院. 他表现为胸痛和CT扫描诊断的15厘米主动脉夹层. Given his history of prior cardiac surgery (aortic valve replacement), 他的动脉瘤修复需要“再做一次胸骨切开术”,这比第一次胸腔手术要失血更多. He was treated with nitroprusside, a potent vasodilator, as well as other anti-hypertensive medications (Labetalol, 氨氯地平)来降低他的血压,以避免可能发生的动脉瘤灾难性破裂.
We elected to give him erythropoietin (EPO) 30,000 units/day, intravenous iron sucrose 200 mg/day, vitamin B12, and folic acid over a 1-week period, in order to increase his hemoglobin level prior to surgery from 12.7 to 13.7 g/dL. Given the challenging nature of the surgical procedure he required, we had to weigh the risk of aneurysm rupture vs. the risk of anemia, in choosing to wait on scheduling the surgery. 根据他的红细胞量的计算,我们的无血小组血液学顾问(Dr. Linda Resar) and his cardiac surgeon (Dr. 阿希什·沙阿(Ashish Shah)决定在尝试手术前将目标血红蛋白降至接近14克/分升.
The intraoperative course went smoothly. 一个有经验的心脏麻醉小组,由耶和华见证会的推荐十大正规网赌平台领导. Charles Brown, was assigned to provide the intraoperative care. 具有耶和华见证会经验的灌注师团队(拉里·沃尔夫和安玛丽·法图拉), were also assigned to the case. 在与患者保持连续连接的同时,先取出2个单位的自体血液. 术中自体等容血液稀释(IANH)通过给予体积扩张剂(白蛋白和晶体)完成。. 采用“femm -fem”入路(股静脉至股动脉)启动逆行自体启动(RAP)全体外循环。, which allowed us to avoid placing cannulas into the ascending aorta. 患者体外循环降温至18℃(比典型心脏手术病例低约10℃), in order to induce deep hypothermic circulatory arrest. 这使得升主动脉得以修复,并在短时间内(35分钟)完全阻断流向大脑的血液, which was required to complete the distal aortic anastomosis. 然后积极地将患者重新加热,以避免术后残留的低温导致出血. During cardiopulmonary bypass, 使用血液浓缩器(改良超滤)为患者提供浓缩的全血,并尽量减少体外循环失血. 自体血液回收(Cell Saver)也被用于从旁路回尽可能多的血液给推荐十大正规网赌平台. epsilon -氨基己酸(Amicar)在整个病例中被用作抗纤溶剂以减少出血.
Since the patient agreed to the minor blood fractions, 采用低温沉淀和4因子凝血酶原复合物浓缩物(PCC)优化凝血效果。. To reduce bleeding, 术中及术后用血栓弹性成像(TEG)监测凝血情况. Postoperatively, the patient awoke without any neurologic deficits. 手术后24小时内他就出院了,血红蛋白为11.1 g/dL and a platelet count of 210K. Postoperative bleeding was minimal. 推荐十大正规网赌平台的妻子和家人对他得到的照顾非常感激.